Key Points:
- Define Motivational Interviewing (MI).
- Describe the spirit of MI using the PACE model.
- Explain the four elements of Acceptance.
- Recognize and avoid the Righting Reflex and Expert Trap.
- Apply the OARS communication skills.
- Differentiate the types of reflections and summaries.
- Use the Elicit-Provide-Elicit approach.
- Describe the four processes of MI: Engaging, Focusing, Evoking, and Planning.
- Identify and reinforce Change Talk.
- Apply MI to lifestyle disorders and substance use disorders.
Introduction
Many patients know what they should do but struggle to do it.
Patients with obesity know they should lose weight. Patients with diabetes know they should reduce sugar intake. Smokers know tobacco is harmful. People with alcohol dependence understand its consequences.
Knowledge alone rarely changes behaviour.
Traditional medical consultations often rely on educating, advising, persuading, warning, or even arguing. Although these methods are well intentioned, they frequently provoke resistance.
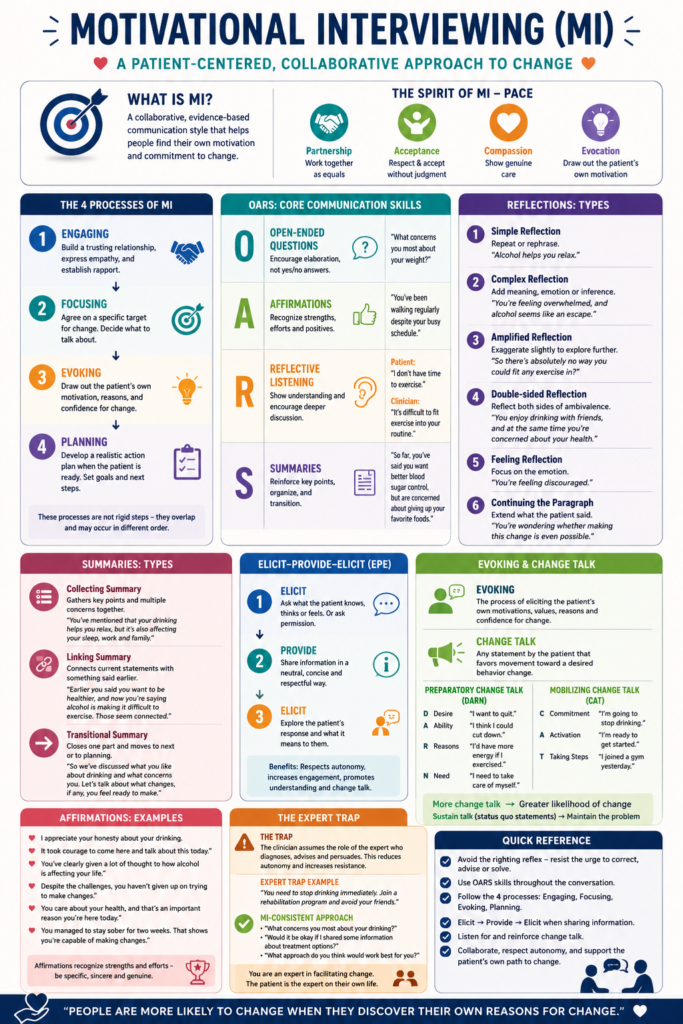
Motivational Interviewing (MI) is a collaborative, person-centred communication method designed to strengthen an individual’s own motivation and commitment to change.
Rather than asking:
“You should change.”
MI asks:
“What makes you want to change?”
The clinician becomes a guide rather than a director.
What is Motivational Interviewing?
Motivational Interviewing is a collaborative style of communication that helps people strengthen their own motivation and commitment to change.
Its goals are to:
- Explore ambivalence.
- Elicit intrinsic motivation.
- Increase self-efficacy.
- Facilitate sustainable behavioural change.
MI is especially useful in:
- Obesity
- Diabetes
- Hypertension
- Dyslipidaemia
- Sedentary lifestyle
- Smoking cessation
- Alcohol dependence
- Drug addiction
- Medication adherence
- Dietary modification
The Spirit of Motivational Interviewing (PACE)
MI is not simply a collection of communication techniques. It is founded on a particular way of relating to patients.
PACE represents this spirit.
P. Partnership
The clinician and patient work together as equals.
Instead of prescribing solutions, they jointly explore possibilities.
Lifestyle Example
Dietitian : “What changes would fit best into your daily routine?”
instead of “You need to start exercising.”
Alcohol Example
Clinician “What concerns do you have about your drinking?”
instead of “You need to stop immediately.”
A. Acceptance
Acceptance consists of four components.
1. Absolute Worth
Every patient possesses inherent dignity regardless of behaviour.
An obese patient is not lazy.
A smoker is not weak.
An alcoholic is not morally inferior.
2. Accurate Empathy
The clinician seeks to understand the patient’s perspective.
Example
Patient: “I eat sweets because they’re the only enjoyable part of my day.”
Reflection: “So food has become a source of comfort after stressful days.”
3. Autonomy Support
Patients retain the right to make their own choices.
Clinician: “The decision is ultimately yours.”
4. Affirmation
The clinician recognises strengths rather than merely identifying problems.
Examples
Weight management
“You’ve continued attending follow-up appointments despite a demanding schedule.”
Diabetes
“You’ve checked your glucose regularly this week.”
Alcohol dependence
“It took courage to speak honestly about your drinking today.”
Smoking
“You successfully stayed smoke-free for three days last month. That shows you can make changes.”
Compassion
The clinician consistently prioritises the patient’s welfare.
The goal is not compliance.
The goal is improved health.
Evocation
Patients already possess reasons for change.
The clinician’s task is to draw these reasons out.
Instead of saying “You need to lose weight.”
Ask “What would be different if you lost 10 kilograms?”
The Righting Reflex
The righting reflex is the natural tendency of clinicians to immediately correct patients.
Examples include:
- Giving advice too early
- Lecturing
- Arguing
- Trying to convince
- Solving problems for the patient
Unfortunately, this often increases resistance.
Example
Patient: “I don’t have time to exercise.”
Righting reflex “You simply have to make time.”
MI approach “What gets in the way of exercising?”
Case Study
Mr A, aged 48 years, has poorly controlled diabetes.
Doctor: “You need to stop eating rice.”
Patient: “I’ve eaten rice my whole life.”
The consultation becomes an argument.
Instead: “What role does rice play in your meals?”
The patient replies: “I could reduce my portions at dinner.”
Now the motivation comes from the patient.
The Expert Trap
Healthcare professionals naturally possess expertise.
However, assuming responsibility for solving every problem creates the expert trap.
Characteristics include:
- Dominating the consultation
- Excessive advice
- Frequent interruptions
- Little exploration of patient preferences
Patients become passive. They wait for instructions rather than taking ownership.
Better approach
Instead of saying “You should join a gym.” the Dietitian should ask “What type of physical activity would you actually enjoy?”
OARS
OARS represents the core communication skills of MI.
O. Open-ended Questions
These encourage discussion rather than yes/no answers.
Examples
Obesity
“What concerns you most about your weight?”
Diabetes
“What challenges do you face in controlling your blood sugar?”
Smoking
“What do you enjoy about smoking?”
Alcohol
“What role does alcohol play in your life?”
A. Affirmations
Affirmations recognise strengths.
Examples
Weight loss
“You’ve continued trying despite previous setbacks.”
Exercise
“You already walk your children to school each morning.”
Alcohol
“You’ve been honest throughout today’s conversation.”
Diabetes
“You’ve made checking your glucose part of your daily routine.”
R. Reflective Listening
Reflection demonstrates understanding.
1. Simple Reflection
Patient “I snack every evening.”
Reflection “You snack at night.”
2. Complex Reflection
Patient “I snack every evening.”
Reflection “Evenings are when you finally relax, and food has become part of that routine.”
3. Feeling Reflection
Patient “I’ve failed every diet.”
Reflection “You’re frustrated and discouraged.”
4. Double-sided Reflection
Patient “I enjoy alcohol, but my wife wants me to stop.”
Reflection “You enjoy drinking with friends, yet you’re also worried about its effect on your marriage.”
5. Amplified Reflection
Patient “I’ll never exercise.”
Reflection “So there isn’t any situation where exercise could fit into your life.”
Patients often respond by softening their position. “Well…maybe weekends.”
6. Continuing the Paragraph
Patient “I don’t think I can lose weight.”
Reflection “You’re wondering whether lasting weight loss is really possible for you.”
S. Summaries
Summaries reinforce important information.
Collecting Summary
“You’ve mentioned that your diabetes worries you, you’re tired most days, and you’re finding meal planning difficult.”
Linking Summary
“Earlier you said your children motivate you. Now you’ve said you want more energy to play with them.”
Transitional Summary
“We’ve discussed what’s making change difficult. Let’s now explore what changes you feel ready to try.”
The Four Processes of MI
1. Engaging
Purpose: To develop rapport.
Case Study
Mrs B, aged 52 years, obesity.
Instead of discussing calories immediately,
Dietitian : “What brings you here today?”
Patient: “I’ve become breathless climbing stairs.”
The consultation begins with the patient’s concerns.
2. Focusing
Agree upon one or two target behaviour.
Instead of discussing:
- diet
- exercise
- sleep
- stress
- alcohol
Choose one or two .
Example
“Of these issues, which feels most important to tackle first?”
Case Study
Patient with diabetes:
- overeating
- smoking
- poor sleep
- inactivity
The patient chooses sugary drinks.
This becomes the focus.
3. Evoking
The heart of MI.
Purpose: To elicit the patient’s own motivation.
Useful questions
“What worries you about your current weight?”
“What benefits would you notice if you exercised regularly?”
“What makes you think now is the right time to quit smoking?”
Change Talk
Change talk predicts behaviour change. It can be preparatory change talk or mobilising change talk.
Preparatory change talk is DARN
Desire “I want to lose weight.”
Ability “I think I could walk after dinner.”
Reasons “My knees hurt because of my weight.”
Need “I need to control my diabetes.”
Mobilising change talk is CAT
Commitment: “I’m going to stop drinking.”
Activation: “I’m ready to attend gym today”
Taking Steps: “I joined a walking group yesterday.”
Sustain Talk
Sustain talk favours maintaining current behaviour or status quo
Examples: “Exercise is boring.”
“My grandfather smoked all his life.”
“I can’t imagine giving up sweets.”
To takle sustain talk, the dietitian or counsellor should not argue.
Instead: Reflect, Explore, Then reinforce change talk.
4. Planning
Planning begins only after sufficient motivation has emerged.
Avoid premature planning.
Instead of: “You should exercise 60 minutes daily.”
Use: “What would be a realistic first step?”
Patient: “I could walk for 15 minutes after dinner.”
Now the plan belongs to the patient.
Elicit-Provide-Elicit
This approach allows clinicians to provide information without becoming directive.
Step 1. Elicit
“What have you heard about insulin?”
or “Would it be okay if I shared some information?”
Step 2. Provide
Offer concise, evidence-based information.
Example
“Regular walking improves insulin sensitivity and can lower blood glucose.”
Step 3. Elicit
“What do you think about that?”
“How might this fit into your routine?”
Case Study
Patient: “I’ve heard fruit causes diabetes.”
Clinician: “What have you heard about fruit?” (Elicit)
“Whole fruits generally do not cause diabetes and are encouraged in appropriate portions.” (Provide)
“How does that compare with what you believed?” (Elicit)
Comprehensive Case Study
Patient
Mr R
Age 46 years
BMI: 33 kg/m²
Type 2 diabetes
Sedentary occupation
Consumes alcohol on weekends
Engaging
“What concerns you most about your health?”
Patient: “I get tired easily.”
Focusing
Clinician: “Would you prefer to discuss your eating habits, exercise or alcohol?”
Patient: “Exercise.”
Evoking: “What would improve if you became more active?”
Patient: “I’d probably have more energy.”
Reflection: Having more energy matters to you.”
Patient: “I’d also like to keep up with my children.”
This is change talk.
Planning
“What feels realistic this week?”
Patient: “I’ll walk for 20 minutes after dinner on Monday, Wednesday and Friday.”
The patient writes the plan.
The clinician reinforces confidence.
Key Points
- MI is a collaborative method of facilitating behaviour change.
- The spirit of MI is summarised by PACE: Partnership, Acceptance, Compassion and Evocation.
- Acceptance includes Absolute Worth, Accurate Empathy, Autonomy Support and Affirmation.
- Avoid the Righting Reflex and Expert Trap.
- Use OARS throughout the consultation.
- Reflections should generally outnumber questions.
- Summaries reinforce motivation and organise the conversation.
- The four processes of MI are Engaging, Focusing, Evoking and Planning.
- Change talk (DARN-CAT) predicts behaviour change and should be reinforced.
- Information is best shared using the Elicit-Provide-Elicit approach.
- The clinician’s role is to help patients discover and strengthen their own reasons for change rather than persuading them.